English Site
This is the outpatient clinic “Ujiie neurosurgical and medical clinic”.
This clinic is operated by consultant neurosurgeon Hiroshi Ujiie and Prof. Akio Hyodou. We are very experienced neurosurgeons’ group.
If you are facing some difficulties such as decision how to treat your intracranial aneurysms or brain tumors or some other disease in brain, please consult our clinic.
We understand that receiving a neurosurgical diagnosis makes you feel anxious and lost. That is all the more reason to get a certain second opinion from knowledgeable neurosurgeons.
At first you can begin to e-mail your information to our clinic.
E-mail: neurosurgery@tbz.t-com.ne.jp
Problem of intracranial aneurysm:
The patients who have been diagnosed with intracranial aneurysm are facing two problems. One is whether the aneurysm will rupture in near future or not, another one is when you have been told that to treat the aneurysm must be very difficult. So, if I were in your position to undergo surgery, it is easy to imagine that I would be concerned about complications from the surgery.
Answer about first problem; unruptured aneurysms have a mortality rate of nearly 50% if they rupture, but the annual rupture rate for unruptured aneurysms is 1% at most. Even with prophylactic surgery, the surgical complications are 2-3%. However, many unruptured aneurysms do not rupture during their lifetime. There must be no need to operate upon an aneurysm that will not rupture in the future. Before you make the decision to have surgery, you need to know whether or not your unruptured aneurysm will really rupture in the near future. We will answer this important question, “to operate or not to operate”.
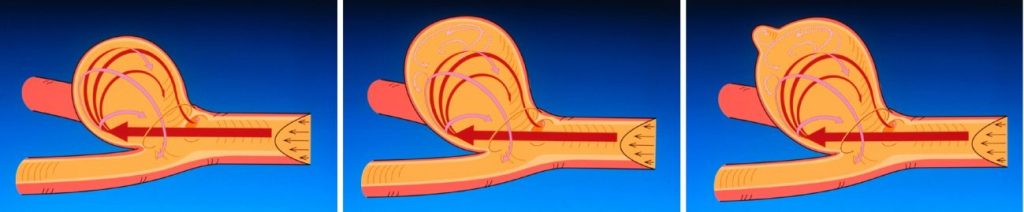
The three pictures are schematic representations of an aneurysm about process of aneurysmal growth, an aneurysm that has grown slightly, and the last one is an aneurysm just before ruptures. In the left picture, you can see that blood stream enters into the aneurysm and flows smoothly along the aneurysm wall. In the middle, however, the flow entering the aneurysm did not go all the way to the bottom of the aneurysm, but instead created a secondary vortex at the bottom of the aneurysm. In the last one, you can see the daughter aneurysm at the bottom of the aneurysm, the wall of the daughter aneurysm is fragile and there is the secondary vortex. The vortex flow is very slow and is almost stagnant. When a daughter aneurysm with fragile wall occurs and the flow stagnates, the aneurysm will soon rupture.
Precise MRI/A images to diagnose this rupture-prone morphology is necessary.
Answer of second problem; the high image resolution of the Icono machine and Prof. Akio Hyodo’s skill to manipulate a catheter and more than anything his enormous experiences of endovascular surgeries made me think that the era of craniotomy for intracranial aneurysms was over and there is no doubt almost all intracranial aneurysms must be treated by endovascular intervention.
I am showing several photos of our institute “Kamagaya General Hospital.
Prof. Akio Hyodo is operating upon.

Treatment scene of endovascular surgery in our hospital using new machine Icono.
The ICA aneurysm was treated by coils shown in left hand side. When the tangle of coil occupied almost 40% of the volume inside the aneurysm, blood flow into the aneurysm completely blocked and thrombosed within short time. Once the blood stops flowing into the aneurysm, full recovery is promising.
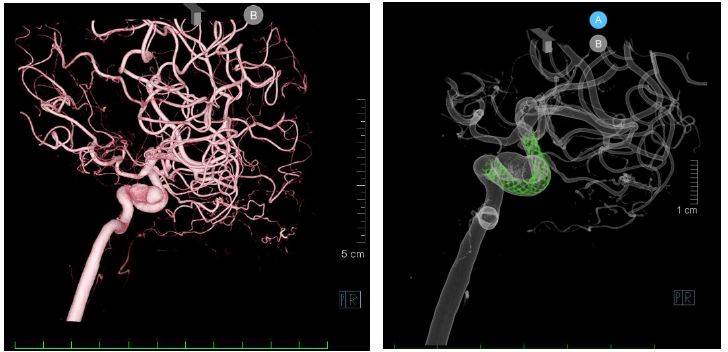
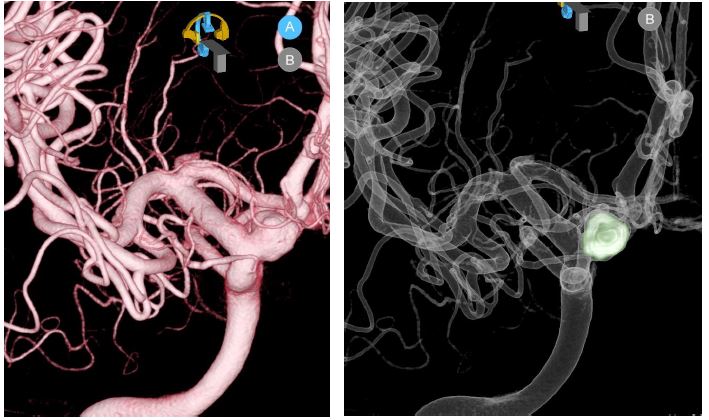
The left figure shows a large internal carotid artery aneurysm in the cavernous sinus and is extremely difficult to treat by craniotomy. However, in this aneurysm, a fine mesh stent called a flow diverter is implanted in the cerebral vessels to reduce blood flow into the aneurysm and promote thrombosis within the aneurysm over time. I love this treatment, because it is an extremely elegant surgical procedure.
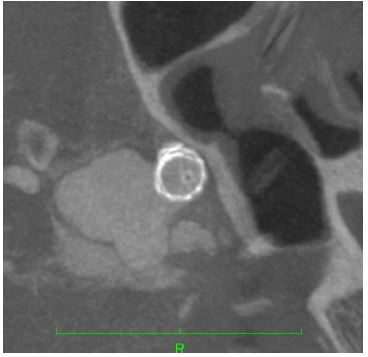
This figure shows a cross-sectional view of the internal carotid artery; Icono can perform CT scans as well as cerebral angiography. As you can see, there is a metal barrier between the vessel and the aneurysm.
Problem of brain tumors:
Brain tumors can be simply classified into benign or malignant. A benign tumor can be completely cured by total removal if possible, but a malignant tumor invades the brain tissue as if it were seeping into it, so when it is removed, a part of the normal brain is also removed, resulting in loss of some neuronal function. Even if the tumor is said to be benign, if it is located deep in the brain, surgery becomes very difficult.
Primary brain tumors include meningiomas (25%), gliomas (25%), pituitary adenoma (20%), and Schwanoma (10%), that account for 80% of all primary brain tumors.
Nowadays, surgeries of brain tumor can be done very safely with preoperative embolization + resection or partial resection + gamma knife. If old fashion craniotomy is considered as an infantry tactic, endovascular surgery and gamma knife are something like bombing by the Air Force. My strategy for treating brain tumors is to use air force bombing to damage brain tumors, and completed by the infantry units.
I will offer you safe and easy but well programed strategy to treat your brain tumor.
In this case, a giant pontine cavernoma extending from the midbrain to the
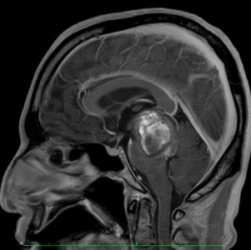
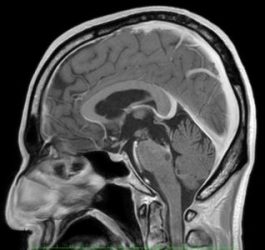
In this case, a giant pontine cavernoma extending from the midbrain to the thalamus is shown. The patient was almost dying because the giant cavernoma was compressing the surrounding important brain tissue such as motor and alarm neuron pathways. The surgeries were performed twice through the supra-cerebeller route. The cavernoma was almost completely removed, and the brainstem recovered well. You can see the plasticity of the pons restoring to its original size. With such a giant cavernoma, it is better to remove it by two staged operations, the first time to reduce pressure on the brainstem, and then remove the entire cavernoma in the second step. He is now still recovering.
We are very experienced neurosurgeons’ group.
If you are facing some difficulties how to treat your intracranial aneurysms or brain tumors or some other disease in the brain, please consult our clinic.